Published on .
The circumstances in which people live, work and spend their free time have an enormous impact on their intrinsic well–being. These social determinants of health (SDOHs), including access to food, housing and transportation; health literacy and educational attainment; income level; and interpersonal relationships, are responsible for up to 80% of clinical outcomes.
The traditional clinical care system is inherently ill-equipped to recognize and address these socioeconomic factors due to misaligned incentives and systemic societal biases.
Fortunately, that fundamental breakdown is changing with the infusion of value-based care into more and more relationships between providers, health plans and regulatory leaders.
Incentivizing MA plans to improve health equity
With measurable health outcomes and improved patient experiences as the pathways to earning financial incentives, health plans and providers now have a much stronger impetus to remove barriers to overall well–being. One such strategy involves architecting socioeconomically informed care programming through value-based benefit design, behavioral interventions and resource connections. And through high-impact performance-based frameworks, such as the Star Ratings system for Medicare Advantage (MA) health plans, institutions like the Centers for Medicare and Medicaid Services (CMS) are leading the industry toward a more comprehensive, structured approach for addressing SDOHs.
For example, the new Health Equity Index (HEI), as a replacement for the previous reward factor, incentivizes qualifying plans to boost their Star Ratings through measured health improvement of vulnerable cohorts within the member population. Certain requirements qualify MA plans for the HEI, including the presence of members with specific social risk factors (SRFs), including:
- Those who receive a low-income subsidy (LIS)
- Those who are dual eligible (DE) for Medicare and Medicaid
- Those who are disabled (defined in this case by CMS as Medicare members under 65 who enrolled in Medicare due to a disability)
How the HEI works
CMS will use a subset of existing Stars measures (announced annually) as part of the HEI to observe the care provided to SRF populations and determine eligibility for incentive rewards. Contracts will be compared to peers, and divided into three buckets, each of which will receive a corresponding positive, neutral or negative score. Those that perform well in this ranked system are eligible to earn up to an additional 0.4 Stars, which can drive an increased overall Star Rating and enhance the likelihood of earning valuable Quality Bonus Payment (QBP) incentive dollars.
As dual eligibility for both Medicare and Medicaid is one of the initial SRFs qualifying a contract for the HEI, Dual Eligible Special Needs Plans (D-SNPs) will likely need to prepare for adequate performance on the included Stars measures. To meet the challenges of this unique member population, perform well on Stars measures that fall under the HEI and unlock financial incentive opportunities through earned QBP, D-SNPs must take a holistic, data-driven approach to identifying and engaging members in adherence with medication and treatments.
Looking to improve performance on the HEI? Check out our white paper for actionable steps!
Why dual-eligible members require a personalized approach to health equity
 The HEI identifies dual eligibility as a proxy measure for socioeconomic vulnerability. Approximately 12.5 million people meet the threshold for dual enrollment, comprising 17% of Medicare beneficiaries and 14% of Medicaid enrollees, according to the Kaiser Family Foundation. They are more likely to report being in fair or poor health (44%) compared to Medicare beneficiaries without Medicaid (17%), and chronic conditions are also more prevalent in this population. About a quarter of DE members reported having five or more chronic conditions compared to just 15% of Medicare-only individuals. Mental health conditions are also much more common, as are intellectual/developmental disabilities, and Alzheimer’s or dementia.
The HEI identifies dual eligibility as a proxy measure for socioeconomic vulnerability. Approximately 12.5 million people meet the threshold for dual enrollment, comprising 17% of Medicare beneficiaries and 14% of Medicaid enrollees, according to the Kaiser Family Foundation. They are more likely to report being in fair or poor health (44%) compared to Medicare beneficiaries without Medicaid (17%), and chronic conditions are also more prevalent in this population. About a quarter of DE members reported having five or more chronic conditions compared to just 15% of Medicare-only individuals. Mental health conditions are also much more common, as are intellectual/developmental disabilities, and Alzheimer’s or dementia.
The result is an extremely challenging population that requires support, such as medication and healthcare appointments, to address health conditions. However, SDOH barriers within the population can make it increasingly difficult to access what’s needed. For example, per the same Kaiser report, almost 90% of DE members live on an annual income of less than $20,000.
Barriers such as these, contributing to worsening health outcomes, are reflected in the Star Ratings performance of D-SNPs. D-SNPs continue to lag in key medication adherence measures when compared to non–D-SNPs. These plans are significantly less likely to achieve 4.0+ Stars for adherence to diabetes medications, hypertension (RAS) medications and cholesterol medications.
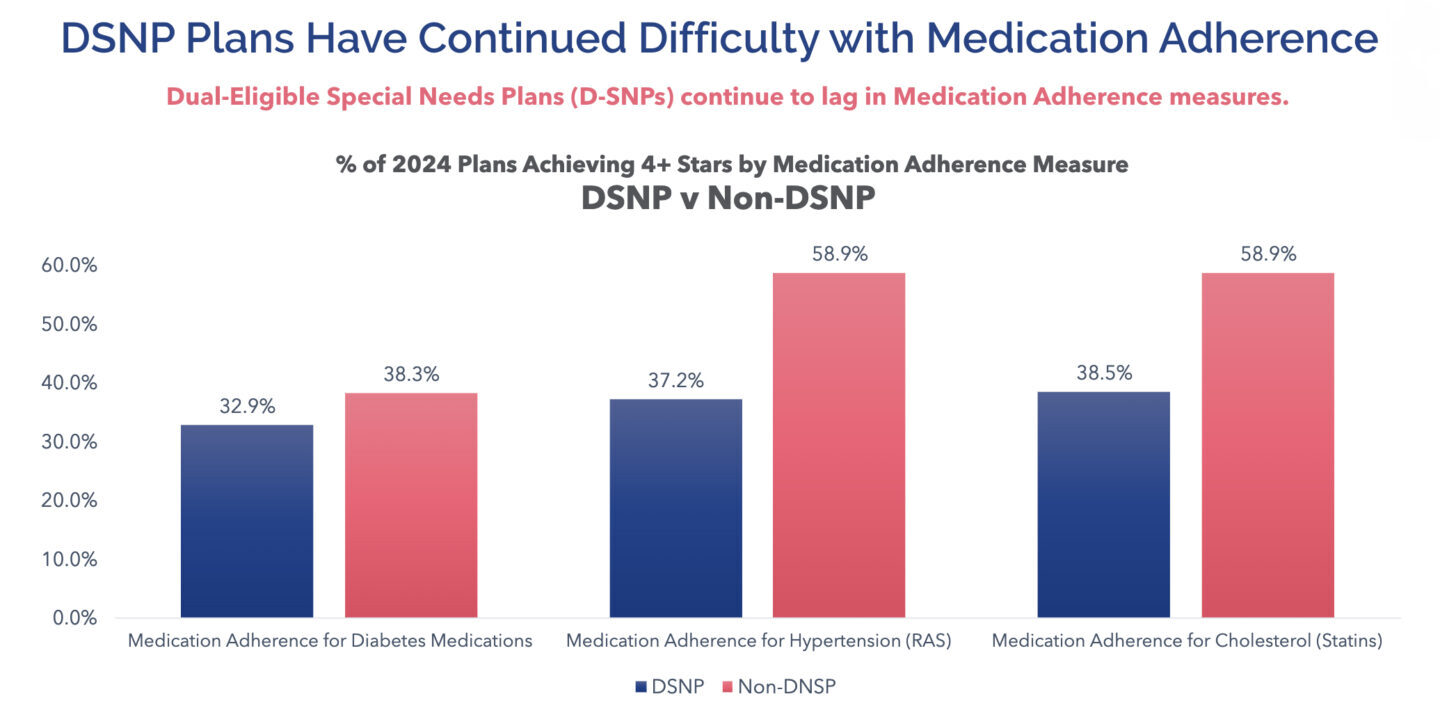 Source: CMS. Part C and D Outcomes Data. Released October 13, 2023.
Source: CMS. Part C and D Outcomes Data. Released October 13, 2023.
This discrepancy is highly problematic for HEI-eligible D-SNPs, since they’ll be compared to their peers on these and other measures before being ranked accordingly. Failing to crack the top third of performance scores on the HEI will restrict access to crucial financial incentives from the QBP.
To boost performance for these highly complex members facing a number of clinical and non-clinical challenges, D-SNPs will have to take a targeted and personalized approach to connecting with members, identifying their individual barriers and applying a variety of innovative solutions to ensure they have the socioeconomic and clinical resources they need to improve their health.
3 ways to improve Star Ratings performance and tackle the HEI
To ensure success with the HEI and catalyze overall higher performance on Stars, D-SNPs will need to merge clinical excellence with SDOH-focused activities. This merger will require plans to develop a data-driven roadmap to socioeconomically informed care, starting with the use of analytics to target the right individuals at the most impactful points of their health journey.
The HEI uses the standardized proxies of dual-eligibility, low-income subsidy and disability status as a clear starting point for identifying members who are likely to have significant barriers to care and may be chronically unengaged in preventive care or health maintenance. But to overcome these multifaceted issues, D-SNPs will need to take the process one step further by getting more granular about their members’ individual challenges and opportunities.
To do so, they will need to implement a technology platform that can generate detailed risk scores by identifying members with adherence and HEDIS gaps, and incorporating SDOH factors and dispositions from previous interventions into the equation. With this powerful technology at their disposal, D-SNPs can begin to take a strategic approach to connecting with harder-to-manage DE members.
Incorporate SDOH barrier resolution as a foundational Stars strategy
D-SNPs cannot simply use existing SDOH datasets to identify that a member may be facing a non-clinical challenge. They also need to confirm with the member that the barrier exists, discover how it truly affects their ability to engage with care and provide active support to help ameliorate the problem.
Incorporating this process into every part of the Stars strategy means training outreach staff in motivational interviewing to uncover hidden concerns, forming strong partnerships with community-based organizations with available resources, and making it simple and intuitive for outreach staff to refer members to these programs within the workflow.
Plans will also need to establish ongoing interactions with DE members at regular intervals to ensure members follow up with referrals, engage in care consistently and get the timely support they need if new barriers emerge.
Utilize tailored techniques to engage the hardest-to-reach members
Members experiencing extreme SDOH barriers may not be able or willing to engage with their health plan in the same way as other members. Challenges may include lack of trust in the healthcare system, low health literacy, primary languages other than English or lack of access/familiarity with technology. Overcoming these issues means employing innovative strategies, such as:
- Timing calls for the beginning of the month when members are more likely to have minutes available on pre-paid cell phones
- Using multi-lingual clinicians to connect with members in their primary language
- Prioritizing real human voices (not IVR) when reaching out to members or leaving voicemails
- Emphasizing offers of support and help rather than focusing on plan-centric actions the member has not completed
Keeping the member’s unique needs in the center of every interaction can break down resistance to engagement and help outreach staff form meaningful, effective relationships with all members.
Focus on a defined set of high-impact Star Ratings measures
Higher performance on certain Star measures is tightly correlated to overall success, which gives D-SNPs a high-value focal point for their efforts. In addition to the annual release from CMS indicating which Stars measures will fall under the HEI, plans can zoom in on measures that can lead to higher over Star Ratings.
There are five key measures in particular that saw significant cut point increases in the 2024 Star Ratings—and are also aligned with 4.0+ Stars performance, per AdhereHealth data. These measures are:
- Controlling High Blood Pressure
- Diabetes Care Blood Sugar Controlled
- MTM Program Completion Rate for CMR
- Care for Older Adults (COA) – Medication Review
- Care for Older Adults (COA) – Pain Assessment
In the 2024 Star Ratings, over two-thirds of D-SNPs achieving 4.0+ Stars for these measures also earned 4+ Stars in overall performance.
Correlation of overall Stars performance to specific measure performance
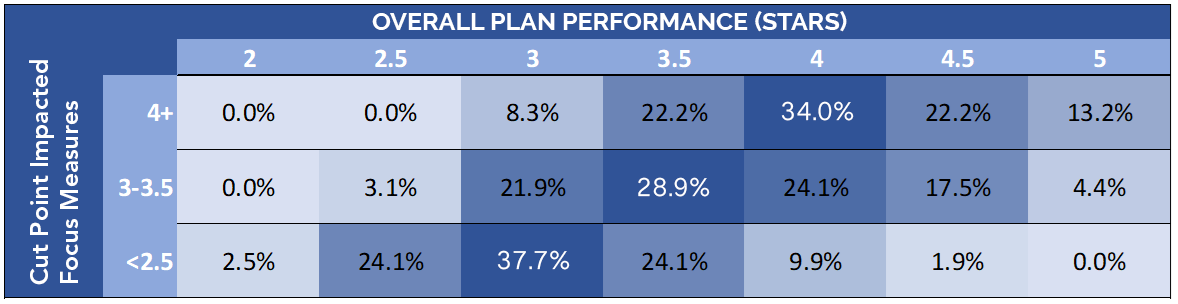 Zeroing in on this group of measures can assist D-SNPs with both HEI performance and their overall scores, while actively helping members to improve their health across multiple chronic conditions.
Zeroing in on this group of measures can assist D-SNPs with both HEI performance and their overall scores, while actively helping members to improve their health across multiple chronic conditions.
In conclusion
The HEI ramps up the competitiveness of the MA environment by requiring eligible plans to outperform their peers with the most vulnerable populations. For D-SNPs that may be falling behind on the measures that matter most for highly complex dual-eligible members, taking an integrated SDOH approach to Stars performance is a must.
D-SNPs will need to enhance their focus on key non-clinical factors affecting their most difficult-to-engage members by leveraging data to illuminate SDOH barriers and employing creative, person-centered strategies to resolve major concerns. By pairing these activities with a focus on high-impact measures with the biggest effect on overall performance, D-SNPs can tackle the challenges of the HEI while positioning themselves for greater financial success in the near future.
For more details about addressing and resolving SDOH barriers to achieve high performance on the HEI, check out our white paper: Improving Performance on the Medicare Advantage Health Equity Index with an SDOH-First Approach to Adherence
 Authored by:
Authored by:
Kempton Presley, MPH, MS
AdhereHealth, Chief Strategy Officer
